




Fibroids / Myoma
What is a myoma?
Myomas, also called fibroids, are non-cancerous tumors on the uterine wall.
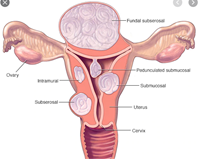
Myomas grow in various sizes and may even grow into large masses that push the uterus and the surrounding organs. It is not rare to see several myomas in one uterus. There are three main types of myomas categorized by their position on the uterine wall.
How common are myomas?
20-40% of women over the age of 35 are found to have myomas!
What causes myomas?
The causes of myomas are still unknown but research points to a connection with:
- Genetics – increased frequency in women with a female relative diagnosed with fibroids.
- Menstruation at an early age.
- Obesity.
- High-fat diet, with a poor intake of fruit and vegetables.
- Hormones, mainly estrogen and progesterone, affect the size of myomas and there is evidence of excess receptors for these hormones in myoma cells. Additional growth factors affect their size.
What are the symptoms for myoma?
- Hemorrhaging, sometimes massively, usually during menstruation.
- Myomas cause infertility in 2-10% of cases.
- Pain and pressure in the pelvis.
- Problems in urination such as urgency and leaking as well as urinary tract infections.
- Constipation.
- Leg and back pain.
How are myomas diagnosed?
Sometimes, diagnosis is accidental during a routine gynecologist examination.
Occasionally, the gynecologist will ask for more tests if there are symptoms of myomas:
- Ultrasound – produces a good picture of the entire uterine cavity and characteristics of the myomas.
- MRI – will produce a reliable picture of myoma size and position and will assist in planning treatment.
- Hysteroscopy – a small telescope is inserted into the uterine cavity for a direct view.
- Additional tests – for instance, blood tests to rule out anemia caused by hemorrhage.
What are the prevalent treatment options today?
If the myoma is small with no significant symptoms, the best option is to wait and follow.
If symptoms are severe and the myomas must be treated, the most common suggestion is partial or total surgical removal of the uterus. These procedures involve risks of anesthesia, long recovery time, and inability to conceive. In addition, myomas recur in 10-30% of the cases during the years following surgery.
Are there other options except for surgical removal?
YES!
- טיפול תרופתי: מוצע לנשים הסובלות מדימומים קשים. תחליפים הורמונליים והתקנים תוך רחמיים נועדו להפחית את הדימומים. אלו לא יעלימו את המיומות באופ•
- Medication: offered to women with severe hemorrhaging. Hormonal supplements and IUDs are intended to reduce hemorrhaging. These options will not completely eliminate the myomas.
- MR guided surgery with US (MRgFUS): ultrasound waves are directed at the tumors for embolization.
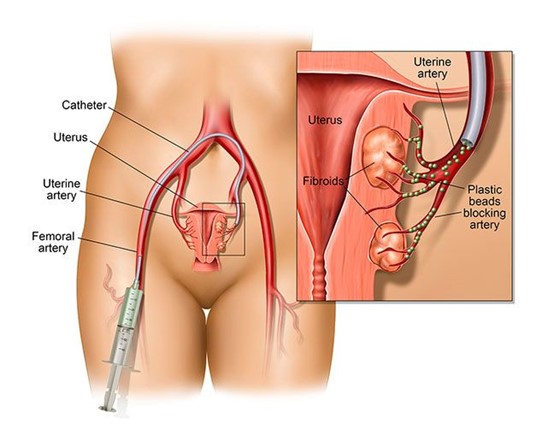
- Minimally-invasive intervention: this procedure is designed to cut-off the blood supply to the tumor, thus causing it to shrink and disappear. This is achieved by closing the artery that feeds the myoma with small particles. The procedure is performed with catheterization through a small incision in the groin or hand, under imaging that provides real-time tracing of the procedure with no need for anesthesia. This procedure is usually completed within 1-1.5 hours.
How is the procedure performed?
The patient, lying down, is monitored for pulse, blood pressure and oxygen levels. The procedure is performed by an interventional radiologist after local anesthesia, usually in the groin area. Mild relaxation medication may also be administered. The doctor will then make a tiny incision and through it insert a thin tube (catheter) to the artery and maneuver it to the treatment site. A small amount of contrast agent is injected for the radiologist to properly view, by imaging, the arteries that supply blood to the myoma and locate where to apply embolization (close them). The surgeon then emits tiny particles that cause an obstruction of the indicated arteries.
By obstructing the arteries, the blood supply to the myoma is cut off and subsequently it will gradually shrink. At the end of the procedure, the catheter is removed and pressure is applied to the incision area.
What is the recovery process?
After the embolization, the patient is discharged the same day of surgery, and may resume normal activity within several days. Dull pain is expected in the lower pelvis area for several days. The pain may be significant on the day after surgery, therefore, the patient will usually stay hospitalized for pain control. The method of pain management will be chosen before the procedure. One of the options is epidural tube insertion (like at childbirth) for administration of analgesics during the first day after treatment.
The myoma gradually shrinks over a period of several months resulting in significant improvement and even disappearance of symptoms.
What are the advantages of this technique?
First and foremost, avoiding surgery and consequential long hospitalization and instead, speedy healing and resuming normal activity.
Second, the success rate in eliminating pain and hemorrhaging is estimated at approximately 90%.
And finally, maximum preservation of future conception possibilities and normal uterine tissue conservation.